CERVICAL CANAL STENOSIS
WHAT IS A CERVICAL CANAL STENOSIS? WHAT IS A MYELOPATHY?
The spinal column is made up of a series of connected bones called vertebrae. Inside them, the spinal cord and its nerves run through the vertebrae in a longitudinal canal, known as the spinal canal.
 |
With age, intervertebral discs become dehydrated, losing height and protruding into the spinal canal, thus reducing the space in it. This loss of height of the discs induces the ligament that joins the vertebrae from behind (the yellow ligament) to lose height, too, and become wider, hence further reducing the space inside the spinal canal. The hypertrophy of facet joints, small joints between each two vertebrae located at their posterior side, also contributes towards narrowing the spinal canal. These changes are collectively called spinal canal stenosis and are common after the age of 50.
|
|
Cervical spondilosis with stenosis of the cervical spinal canal
|
Spinal canal stenosis may evolve at a slow or at a fast rate, but in all cases it ends up inducing the compression of the spinal cord or its nerve roots, altering its functions. Cervical canal stenosis is the narrowing of the cervical spinal canal, whereas cervical myelopathy is the cervical spinal cord lesion that induces this stenosis.
 |
 |
|
Normal cervical spinal canal
|
Cervical canal stenosis
|
 |
 |
|
Normal spinal cord inside normal cervical spinal canal
|
Compressed and distorted spinal cord inside a stenotic cervical spinal canal Compressed and distorted spinal cord inside a stenotic cervical canal
|
WHAT ARE THE SYMPTOMS OF CERVICAL CANAL STENOSIS?
Cervical canal stenosis does not always cause symptoms. Half of the patients show pain in the neck or arms and loss of strength in the upper or in the lower limbs. The upper limbs may show weakness, stiffness or clumsiness in the hands (such as being unable to button a shirt, turn a doorknob or open a jar). Symptoms in the lower limbs may include weakness, frequent falls and/or the need to use a cane or walker. Urinary urgency, when the need to go to the toilet is unbearable and, if it is ignored, the urine escapes, may also crop up. In very advanced cases, bladder and bowel incontinence may occur.
 |
 |
|
Cervical root compression inducing pain in the arm
|
Spinal cord compression with myelopathy
|
The progression of the symptoms varies. Sometimes, the decline is slow and steady; others, symptoms only progress to a certain point and then become stable; and in some cases, they progress rapidly or by leaps, in an irregular fashion.
HOW IS CERVICAL CANAL STENOSIS DIAGNOSED?
Diagnosis is made based on the symptoms and a neurological examination. It is very important to do an early diagnosis to prevent irreversible lesions, such as:
- Abnormal increase of the reflexes in knees and ankles, sometimes accompanied by a repetitive movement known as clonus. The plantar reflex of the feet happens in extension instead of in flexion.
- Reduction of the reflexes in the arms with apparition of a reflex in the fingers known as Hoffman’s reflex.
- Dragging feet.
- Loss of sensitivity in hands and/or feet, sometimes making it difficult to button a shirt or realise a change in the position of the feet.
The range of movement and flexibility of the neck usually diminishes with age and does not necessarily indicate the presence of disorders in the spinal cord or its roots.
Plain X-rays of the cervical column may help suspect the presence of cervical canal stenosis but the best imaging test is MRI, for it does not only show the vertebrae and intervertebral discs, but also allows us to assess the state of the spinal cord and the degree of compression that it is suffering from. CT scans allow us to see the bone better, but not the nervous tissue. However, if a contrast agent is injected into the spinal canal (myelography) the degree of compression of the spinal cord can be assessed.
 |
 |
|
MRI image of cervical canal stenosis with signs of spinal cord lesion
|
MRI image of cervical canal stenosis with signs of spinal cord lesion
|
Electrophysiological studies allow us to distinguish between cervical myelopathy or radiculopathy and other conditions. Electromyography (EMG) analyses the speed of conduction of the nerves, thus allowing us to reveal if the nerves are entrapped and where they are entrapped. Somato-sensory Evoked Potentials (SSEP) allow us to assess the conduction in the nervous pathways of the spinal cord. An alteration in SSEP would indicate that those pathways are damaged; and SSEP can also help us rule out other disorders that may be confused with myelopathy.
TREATMENT OPTIONS
In mild, slow-evolving cases in old patients, conservative treatments may be suitable. In cases of progressive weakness, pain or disability, surgical treatment is recommended.
Medication is used to reduce the pain, muscle spasm and other symptoms. Make sure you tell us about ALL the medication that you are taking, even natural medicines or medicinal herbs, as well as any allergy or adverse reaction to medication that you have had in the past. Be aware that analgesics have usually side effects on the stomach and have to be taken with a gastric protector, and corticosteroids are very powerful anti-inflammatory agents, taken orally or intravenously, that may unfortunately cause much more severe symptoms if taken for prolonged periods of time.
Conservative treatment can relieve the pain and improve quality of life, but it neither halts the evolution of the condition nor corrects the problem of the already-established spinal cord lesion.
Patients with cervical myelopathy gradually reduce their activities, thus reducing too their flexibility, strength and cardiovascular resistance. Physiotherapy helps recover the flexibility in the neck, trunk and limbs, and to control daily activities, especially postural changes when sitting, standing up, having a bath, getting dressed, opening doors, turning keys inside locks, opening and closing jars, using phones and computers…
Structural changes in the patient’s house may be necessary. Maybe the washing machine, the dryer or the cooking plate have to be moved to a more convenient place, and a commode may be useful beside the bed. Transport alternatives may also be considered.
WHEN IS SURGERY NEEDED?
If the disease progresses, it is better to perform surgery before their level of deterioration makes the procedure useless. Unnecessarily delaying the surgical procedure can only bring problems in the future: usually, once the cervical myelopathy has been established, all treatments, even surgery, may only stop the progression of the condition but not improve or reverse the already-established sequelae.
Surgery can be performed from the front of the neck (anterior approach) or from the back of the neck (posterior approach). It will always involve removing bone, disc or ligaments to increase the space in the spinal canal, thus removing the pressure on the spinal cord and its roots. Usually, it will involve too some type of stabilisation (fusion) of the affected areas. Inserting metal implants to support the vertebrae while bone fusion takes place might be recommended. In this case, if the anterior approach is chosen a metal plate will be placed on the spinal column, whereas if the posterior approach is prefered a scaffold of screws and bars will be inserted instead. In specific cases, a combined postero-anterior approach may be necessary. In relatively young people, a discal prosthesis may be implanted, but it is not recommended if there was a previous history of neck pain because the increase in mobility might also increase the amount of neck pain.
After the procedure, an external immobilising system (cervical collar or similar) is sometimes used.
 |
 |
|
Anterior cervical approach
|
Posterior cervical approach
|
SURGICAL OPTIONS
Several factors must be considered when deciding on the surgical procedure. Typically, they will include spinal column alignment, location of the stenosis (front or back), bone quality, number of affected levels, and the patient’s general condition. Based on these factors, an anterior, a posterior or a combined postero-anterior approach will be the most suitable.
Anterior approach surgery is performed through the front part of the neck, and two similar but different procedures may be recommended. Anterior cervical discectomy with fusion involves removing the disc and bony spurs that are compressing the spinal cord and then replacing the disc with a bone graft. It can be performed at one or more levels, but if there is more than one level involved a corpectomy might be recommended. This involves the removal of the vertebral body and the adjacent two discs and inserting a bone graft to stabilise the spine.
 |
 |
|
Surgical exposure of the cervical column in anterior approach
|
Surgical milling of osteophytes that compress the cervical spinal cord
|
 |
 |
|
Surgical removal of osteophytes that compress the cervical spinal cord
|
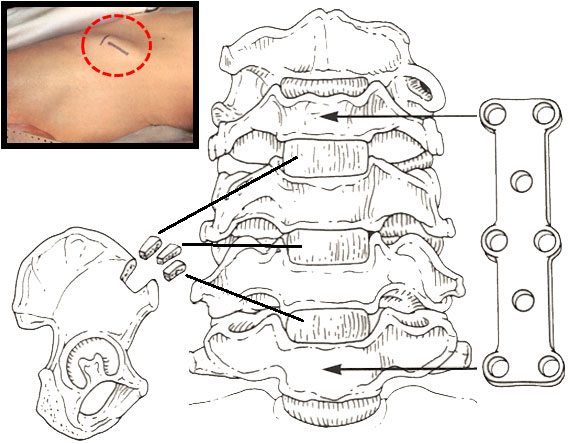
Iliac crest bone graft with metal plate inserted during surgical decompression of cervical canal stenosis
|
 |
 |
 |
|
Frontal view during cervical corpectomy with bone graft and metal plate insertion to treat cervical canal stenosis
|
Lateral view during cervical corpectomy with bone graft and metal plate insertion to treat cervical canal stenosis
|
Lateral view in multilevel cervical corpectomy with bone graft and metal plate insertion to treat cervical canal stenosis
|
 |
Posterior approach surgery, on the other hand, is performed thought the back of the neck, and two common procedures are laminectomy and laminoplasty, both of which remove the pressure from the spinal cord and its nerve roots. Laminectomy involves the removal of the rear elements of the vertebra, also known as laminae. Laminoplasty, however, does not involve removing the laminae but only lifting them up, like a hinge, to increase the space through which the spinal cord runs, thus relieving the pressure on it.
|
|
Posterior cervical approach
|
 |
 |
|
Normal cervical canal
|
Stenotic cervical canal
|
 |
 |
|
Normal cervical column seen from behind
|
Cervical laminectomy
|
 |
 |
|
Laminectomy to treat cervical canal stenosis
|
Laminoplasty to treat cervical canal stenosis
|
 |
 |
|
MRI sagittal section image of cervical canal stenosis: pre-operative state
|
MRI sagittal section image of cervical canal stenosis after laminoplasty
|
 |
 |
|
MRI axial section image of cervical canal stenosis: pre-operative state
|
MRI coronal section image of cervical canal stenosis after laminoplasty
|
After surgery, the patient will remain in the hospital for a few days. Occasionally, a postoperative rehabilitation program is prescribed to promote recovery.