VERTEBRAL FRACTURES
WHAT IS A VERTEBRAL FRACTURE?
 |
A vertebral fracture happens when one or more vertebrae are fractured, with the consequent loss of stability of the spine. The displacement of bone fragments or a possible hematoma, resulting from the fracture, can compress the spinal cord and/or its nerve roots, causing a loss of sensitivity and strength in the legs and/or arms. Occasionally, the cause of the fracture will be an accident (traffic, sport, fall from a significant height…), or to the existence of tumours that destroy and weaken the bone tissue of the spinal column.
|
|
Fracture-dislocation of C5-C6 with cervical spinal cord injury
|
HOW IS A VERTEBRAL FRACTURE DIAGNOSED?
Diagnosis is carried out by means of clinical examination and a neurological exam. It is then confirmed using neuro-imaging tests (spinal column X-rays, CT scan, MRI scan) and, sometimes, using neuro-physiological tests.
 |
 |
|
MRI image of fracture-dislocation of C5-C6 with cervical spinal cord injury
|
Compression fracture of the thoracic spinal cord with spinal cord injury
|
WHEN IS SURGERY SUITABLE?
 |
Surgery is recommended to decompress the spinal cord and its nerve roots, allowing recovery of the lost nervous functions: sensitivity, movement, bladder and bowel control… Ideally, surgery should be performed as soon as possible to maximise the chances of recovery. Once the nervous tissue has been decompressed, the spinal column must be stabilised using bone grafts, either from the patient or made up of another osteogenic material, and reinforced using a scaffold of screws and bars that will hold the spine while the bone grafts fuse. It is essential to understand that the key point of this procedure lies in the fusion of the bone grafts, for the scaffold of screws and bars will eventually fail over the years if there is not an appropriate bone graft fusion. To ensure an appropriate bone graft fusion, smoking and excess weight must be avoided, and the intake of non-steroidal anti-inflammatory agents must be reduced. In most cases, the objective of the surgery is to cure. Nevertheless, at times it is only sought to stabilise the symptoms and relieve the pain as much as possible. Patient that have had surgery once might require in the future new procedures on the same or other levels of the spinal column. |
|
Vertebral fracture with spinal cord compression
|
WHAT WILL HAPPEN DURING A SURGICAL PROCEDURE?
Surgery involves removal of the bone fragments that are compressing the spinal cord or its roots, thus liberating the compressed nervous structures. The posterior approach involves a quite extensive incision due to the fact that it must include, not only the area of the fracture, but also at least 2 or 3 vertebrae above and below it to have good anchorage points (on healthy vertebrae) on which to place the screws. Other times the approach is anterior and carried out though the thorax or through the abdomen, depending on where the fracture is.
 |
 |
 |
|
X-ray image of a fracture of C4 and C5
|
X-ray image of 360° arthrodesis to treat fracture of C4 and C5
|
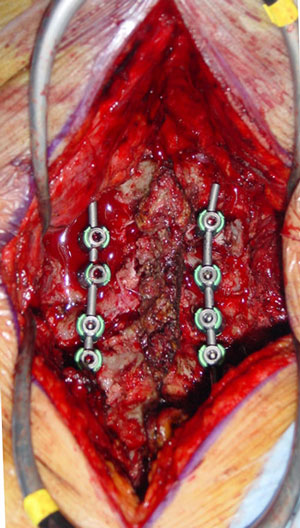
Intra-operative picture of posterior cervical arthrodesis to treat fracture of C4 and C5
|
In selected cases, the vertebral compression fracture can be treated with a vertebroplasty, with or without an arthrodesis with screws and rods.
POSTOPERATIVE RECOVERY
After the procedure, the patient can remain a while in the area of post-anaesthetic recovery to wake up, and then return to their room. Other times, when the patient’s general condition is worse and the vertebral fracture is more severe, they will go to the Intensive Care Unit (ICU). Hospital stay is usually 10-20 days, during which the patient will receive daily cares regarding the surgical wound, medication, postural changes, vital sign monitoring and beginning of rehabilitation. Usually, the pain in the area of the fracture diminishes or disappears after the procedure, only remaining the temporary discomfort due to the surgical wound on the back. The recovery of the lost functions (sensation, movement, bowel and bladder control) can take a long time and, occasionally, will never happen or happen only partially.
WHAT ARE THE RISKS?
The risks of the procedure are those of any surgical procedure: reaction to anaesthetics, infection, bleeding. Any previous illnesses will determine the postoperative period and subsequent evolution.
Intra-operative or postoperative complications may appear and further aggravate the patient’s neurological condition, increasing their paralysis or their loss of movement. The neurological deficits (paralysis, …) may require rehabilitation for months or even years.