SURGICAL TREATMENT OF SPASTICITY
Spasticity is involuntary simultaneous contraction of opposing muscle groups (eg, the flexor and extensor muscles of an arm or leg). This results in severe stiffness of one or more limbs, making it difficult or virtually impossible the movement of affected limbs.
Causes of Spasticity
They are grouped into two main groups:
- Lesions in the brain (cerebral hemorrhage, stroke, multiple sclerosis (MS), brain tumors, etc.)
- Spinal cord injury (trauma, spinal cord tumor, multiple sclerosis, etc.).
Symptoms
Spasticity can cause pain (due to high muscle tension and posture twisted) and interfere with the patient when trying to stay sitting, lying or movint to or from the wheelchair. Also, can hinder patient management and even personal hygiene. In extreme cases it can induce the appearance of skin ulcers as the patient always rests on the same spots.
Treatment
Spasticity is initially treated with physiotherapy, rehabilitation and medications. Among the highlights drug baclofen. When medical treatment is not enough surgical treatment arises. This aims to eliminate the possible spasticity and painful spasms that often accompany it, thereby improving the functioning of the patient (within the limitations of existing disability) and to improve the management for the caregivers. These treatments have no curative effect on the course and severity of the injury to the spinal cord or brain tissue that is the cause of the spasticity. Surgical treatment of spasticity is usually used when all other treatment modalities have failed. There are several possible operations, and the choice depends on the cause and degree of spasticity. In the treatment of spasticity should be aware that certain stiffness may be useful as support when standing. The complete elimination of spasticity would be the loss of this function can support, so that mobility and patient autonomy does not increase but decreases. Possible surgical treatment options are:
- Intrathecal baclofen. As you increased the dose of oral baclofen, there comes a time when side effects appear. These side effects may be a problem and make neccesary to consider other treatment options. The best way is to administer the same drug in the sack where the spinal cord is. This takes place through an infusion pump that is implanted under the skin and the drug goes through a tube until reaching the sac of the spinal cord or thecal sac. About every month and a half the patient must go to the hospital to recharge the pump with baclofen. Its main advantage is that it is reversible and is adjustable. The dose may be increased or decreased with a computer program. The disadvantage is that it does not work well for asymmetric cases (one leg is affectes but the other is not) or when spasticity affects more arms than legs.

 Drug infusion pump (Baclofen)Drug infusion pump (Baclofen)
Drug infusion pump (Baclofen)Drug infusion pump (Baclofen) - Posterior selective dorsal rhizotomy. It consists of partially sectioning the posterior root of the affected spinal segments. Previously it is verified by intraoperative electrophysiological studies which part of the posterior root is more related to the spasticity, and thus, it has to be sectioned. It is especially useful in spastic diplegia in children. It is also usefullin upper limb spasticity.

 Patient positioning for selective posterior lumbar rhizotomy for spastic diplegiaElectrophysiological recording equipment for selective posterior lumbar rhizotomy
Patient positioning for selective posterior lumbar rhizotomy for spastic diplegiaElectrophysiological recording equipment for selective posterior lumbar rhizotomy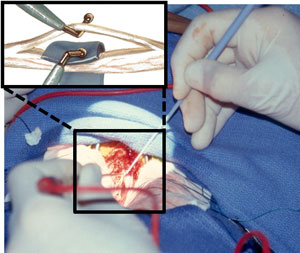
 Selective stimulation of each of the fascicles of each dorsal root to identify those associated with spasticitySection of each root fascicles later related to spasticity
Selective stimulation of each of the fascicles of each dorsal root to identify those associated with spasticitySection of each root fascicles later related to spasticity - DREZ-otomi. It consists of sectioning the fibers of spasticity and pain at the point of entry into the spinal cord. It is useful because it leaves a foot foot pain sensitivity and that can cause injuries to walk (not note that tighten the shoes or to have blisters). It is especially useful for spasticity of the hand.


 DREZ lesion scheme for treatment of spasticity (the black arrow indicates the point of the surgical lesion)Cross section of the spinal cord with an arrow pointing to the point of injuryIntraoperative image of DREZ lesion for treatment of spasticity
DREZ lesion scheme for treatment of spasticity (the black arrow indicates the point of the surgical lesion)Cross section of the spinal cord with an arrow pointing to the point of injuryIntraoperative image of DREZ lesion for treatment of spasticity - Anterior rhizotomy. It consists of sectioning the anterior roots of spinal segments affected. The downside is that a member leaves completely paralyzed, because it is rarely used.
- Myelotomy. It consists of making a longitudinal cut in the spinal cord transecting fibers responsible for the spasticity. Eliminates all reflex arcs. Only used in severely ill patients in whom walking is not going to be possible.
Lateral longitudinal myelotomy for the treatment of spasticity
Posterior longitudinal myelotomy for the treatment of spasticityRadiofrequency myelotomy for the treatment of spasticity - Cordotomy. Consists of completely severing the spinal cord. It is usefull in cases of spinal cord injury in which complete recovery is not possible, but even so is a method that is seldom used .
- Cordectomy. This is the removal of a portion of the spinal cord. This treatment is done only in some patients unresponsive to other treatments. The result of this operation is a total flaccid paralysis below the level of the operation.
- Stereotactic thalamotomy. This involves making an injury to a deep part of the brain, the thalamus, with the help of an electrode and a device that lets us know precisely at what point is the tip of the electrode. This treatment can be effective in congenital spasticity due to brain injury. It is also used in cases of torsion dystonia.
- Selective neurotomy. Involves removing part of the nerve involved in spasticity. For example, removes part of the posterior tibial nerve in cases of foot drop on one side. They are especially useful in cases of localized spasticity in the limbs and reduced extension(foot, hand, …).